As soon as these two came in to see me, I was searching my memory for pediatric and genetic syndromes. When I asked what is wrong, the mom replied “oh she is fine, she is a happy girl.” The mother was the one with complaints of GI upset and musculoskeletal pain.
After addressing those problems, I switch gears to talk about her daughter

and find out that the child is being well taken care of, meeting milestones slightly delayed but progressing well, is eating well, and interacting with others. She was such a beautiful girl, smiling at me from across the table. She was curious, inspecting the stethoscope as I listened to her heart and lungs. Her dexterity is limited to pincer grip on account of her fused fingers, nonetheless, she seems to do just fine with some adaptions. Throughout the exam the child was interactive, smiling, and happy as any other.
My first guess (and without the luxury of further testing or a textbook reference) was a genetic defect called
Treacher-Collins Syndrome, also known as mandibulofacial dystocia (meaning multiple cranial and facial developmental abnormalities). Initially i thought this because of her macrocephaly (large head) and proptosis (bulging eyes), but that doesn't really explain fused fingers and toes. On further review back on the ship I'm thinking more along the lines of
Apert Syndrome or
acrocephalosyndactyly [read: hand and head bone fusions]. This is very rare syndrome (occuring de novo in 1 in 650,000) most often caused by a mutuation of immunoglobulin
FGFR2 (fibroblast growth factor receptor 2), which maps to chromosome bands 10q26, and when altered and upregulated, leads to developmental increased bone matrix formation and premature ossification. The hand fusions create mitten-hands (or syndactyly) are easy to see as pictured, but there is also synonychia (or fusion of the nailbeds), and shortening of the humerus. Developmentally when we think of the bones and fissures of the cranium (
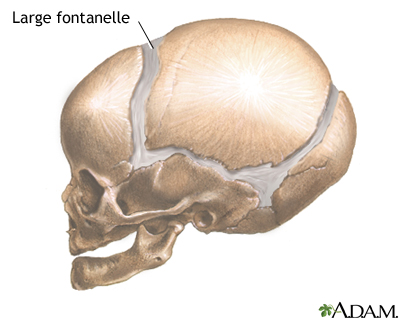
like plate tectonics of the earth -- think in reverse chronology of the continents now moving towards Pangaea) fusing too early (remember the soft spot [ie. fontanelle] of a baby? that is a gap of the coronal cranial plates prior to their fusion, which allows the skull to grow in proportion to the developing brain--you wouldn't want the brain box to close while the contents are still expanding) we see the evidence of this in the morphology (shape) of the head. If
premature closing does happen of some of the fissures, the growth of the brain causes expansion in other directions (usually of the unclosed fissures) which causes macrocephaly [read: large head] in one dimention (in this case coronal sutures probably fused first) and sometimes associated proptosis or exopthalmos (eye bulging) as there are actually 7 bones that fuse to make up the eye sockets.

I pontificate and regurgitate all of this into text simply out of curiosity. I wasn't able to give the mother a name to her daughter's diagnosis at the time, nor am I positive this is correct. In a lot of ways it doesn't matter. In the US, this child would be followed by multiple specialists from neurologists, surgeons, geneticists, pediatricians, ENT, opthamologists, dentist, orthopedist, etc, etc. Here she has only the family doctor that she hasn't seen in the last year or two. But sometimes its not about fixing every problem we see, taking every child and making them look and funciton like every other child. We could not dream to be able to provide such services and long term care to her, we simply will not be in PNG long enough, or have the resources to do all that would be done in the states. But we have to remember what is MOST important. For this girl a happy life with a supportive family and community is the best prognostic indicator that can be assessed. Her hope relies on the smiling faces that surround her rather than serial intercranial pressure monitoring or ventricular shunting surgeries that could be done.
Often times we see these children and think to ourselves in horror, “how horrible!” ...And it's true, it is a tough lot that was given her, being different from her peers. But she is in so many more ways more similar than different. Her metal abilities and cognition are delayed but likely positively affect her level of happiness. Its hard to look past appearances in life, and see through our first impressions. The outside world can be cruel and difficult, but this girl is growing up in an incredibly supportive and loving family that takes excellent care of her. She is luck to have such great parents, and they are just as lucky to have such a sweet little girl. I was so happy to see her today, to know that her mother was not embarrased to bring her into public, to know she is being well cared for, to see that the child is happy and interactive, to have gotten to know these two for the brief time that I did.
At the end of the physical, I was left with a dilemma. There are times when you don’t know what to prescribe. For me this happens quite a bit, but often I can pull out my pharmacopedia or Sanford antimicrobial guide and get a professional opinion. There are other times when there is nothing you can prescribe to make things better. This was neither of those times. This time it was a sour apple and watermellon Jolly-Rancher candy, which brightened this beautiful girl’s day.
Bon Voyage,
~Nic














 Now, I don't want to make all my posts about sad stuff, but that right there is pretty tragic. If the people are afraid of their own health care system, how can they be expected to seek care when they need it? I guess the answer is, they don't.
Now, I don't want to make all my posts about sad stuff, but that right there is pretty tragic. If the people are afraid of their own health care system, how can they be expected to seek care when they need it? I guess the answer is, they don't.

































{kind=link}
{kind=link}
{kind=link}